 A fairly recent longitudinal study of older people with hearing loss that was conducted by John Hopkins University discovered that, over a period of 10 years, people who entered the study with any form of hearing loss showed a much faster rate of brain atrophy – hearing is a neurological process that takes place in the left and right auditory cortices located in the frontotemporal region of the brain – than people who had entered the study with normal hearing.
A fairly recent longitudinal study of older people with hearing loss that was conducted by John Hopkins University discovered that, over a period of 10 years, people who entered the study with any form of hearing loss showed a much faster rate of brain atrophy – hearing is a neurological process that takes place in the left and right auditory cortices located in the frontotemporal region of the brain – than people who had entered the study with normal hearing.
As the ability to hear is impaired, several things happen neurologically that lead to cognitive decline and the development of dementia.
First, as the brain has to devote more resources to concentrate and focus on auditory processing to try to make sense of auditory input, thinking and memory are compromised.
Second, because impaired hearing leads to faulty understanding, communication problems increase as high-frequency sounds become more difficult to distinguish.
My mom was hearing-impaired for most, if not all, of her life. She was fitted with her first hearing aids when she was in her twenties.
Mama was as smart as a whip and mastered reading lips early in her life, instinctively compensating for and making almost imperceptible to most people that her hearing was impaired. The only time she had trouble learning or following instructions was when her back was turned to the people who were talking to her.
She was blessed that Edgar Stohler, the administrator at the old Memorial Hospital in Johnson City, TN, where Mama was training when she was dismissed from the nursing program at East Tennessee State University, recognized that Mama had a hearing loss that was the only thing impeding her success in education and life.
Mr. Stohler advocated for Mama and got her the vocational rehabilitation access and resources she needed – which included hearing aids – and helped Mama to get into another medical-degree program at Duke University where the pressure and ability to hear and respond immediately was not as urgent as surgical nursing would have been.
Daddy learned, as we kids did, how to interact with Mama well, learning what kind of words – those with a sound in the high-frequency range were always most difficult for her to distinguish and understand and her speech reflected that – to either spell out, enunciate more clearly, or avoid altogether in our speech and we all knew to be the second set of ears for Mama where we were present with her.
As an inset to this post, for educational purposes, I’m including the following information to help anyone reading this to both understand how most hearing loss works and which words are most commonly misunderstood by people with hearing impairments.
Human speech is calculated within a frequency range (known as the Speech Banana):
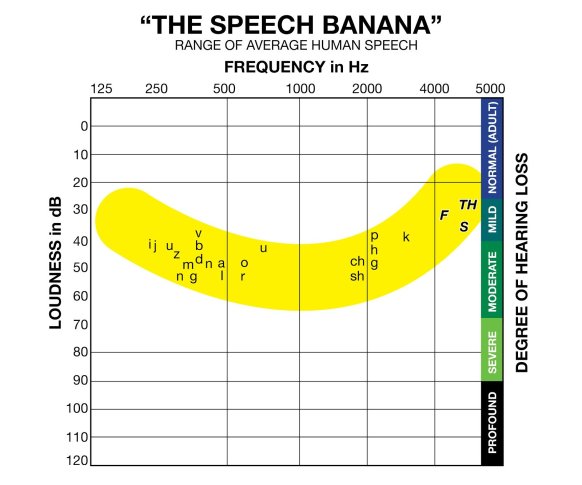
The Speech Banana shows the high frequency (4000 Hz and up) sounds we use in our everyday speech such as f, th, and s (f and s as letters and sounds are often indistinguishable for people with high-frequency hearing loss, and they can’t hear the th sound well enough to know whether the h is silent or not, so they generally use the hard th sound, no matter what).
Although there are other types of hearing impairments, the most common type of hearing loss is a high frequency hearing loss. This is also the type of hearing impairment that generally is manifested earliest.
To increase the overall understanding of someone who is hearing impaired, we should try to replace (eliminate, if possible) high frequency words and sounds (on the right side of the Speech Banana) with easier-to-understand low frequency words and sounds (on the left side of the Speech Banana).
Here’s a common word list of low-frequency words to use instead of their high-frequency counterparts when we are communication with our hearing-impaired loved ones (it requires extra time to think about what and how we’re going to say something, but it seems to me in this unfiltered whatever-pops-in-my-head-I’m-going-to-let-come-out-of-my-mouth world we now live in, taking a little extra time before we put our mouths in gear is not a bad thing):

Mama’s hearing continued to decline throughout her life, but hearing aids helped more than not, for the most part, until her hearing impairment and dementias collided.
One of the first overt signs I observed – although I didn’t know exactly what it meant at the time – was that she stopped putting her hearing aids in as soon as she got up and got washed and dressed when she was in the independent living retirement community.
It would not be until I came every day, usually between 9 am and 10 am, that Mama would put them in so she could hear me.
This led to greater social isolation for Mama, which also puzzled me (but this is the third factor in the hearing-impairment/dementia link), because Mama was an extrovert and liked to get out and talk to her neighbors throughout the day.
This led to the fourth factor, auditory deprivation, which led to an acceleration in the fifth factor in the hearing-loss/dementia link, which is brain atrophy.
Brain atrophy, of course, leads to some degree of dementia (Mama already had the dementia processes of vascular dementia, Lewy Body dementia, and Alzheimer’s Disease in progress, but I am inclined to believe that the hearing impairment aspect played a part in the rapid seven-month decline she experienced in 2010).
 Interestingly, while the John Hopkins University study focused on older people and hearing loss, the University of Wisconsin performed a similar study on late middle-aged adults and found the exact same correlation between hearing impairment and cognitive decline.
Interestingly, while the John Hopkins University study focused on older people and hearing loss, the University of Wisconsin performed a similar study on late middle-aged adults and found the exact same correlation between hearing impairment and cognitive decline.
What this study also found was that the more severe the hearing impairment was, the greater risk the participants had of developing dementia.
While it’s clear that at some point hearing impairment and dementias meet, treating hearing loss early with hearing aids and monitoring hearing ability with appropriate progressive treatment, as need, can be beneficial in delaying cognitive decline and the onset of dementias.
This is something we all should include in our health care programs and address as the need arises. While other odds may be stacked against us for the likelihood of developing dementia, this is one area where we can take preventative measures today to allay this as a culprit of decline in our own neurological health.

Have not read article yet but it hit a note with me! I lost my husband last year after cognitive impairment. He was diagnosed with Parkinson’s Plus, with possibility of Corticobasal degeneration. Not sure when it all began, but he started wearing hearing aids up to 10 years or more before his death.
Pingback: Longevity Briefs: Understanding The Link Between Dementia And Hearing Loss - Gowing Life
I have severe tinnitus which is a distraction in my daily life and especially at work and most definitely with all the multi tasking. my cognitive skills are affected with memory being the number one issue. I have an appointment with the neuroscience dept at our local hospital..hopefully get to the bottom of the memory issues and praying for a good outcome. Our father had alzheimers when he passed away with pancreatic cancer. I’m only 65.
Pingback: Can Ear Infection Cause Brain Fog Symptoms? -