Click below on the new infographic I created to see it in normal size.

Click below on the new infographic I created to see it in normal size.

Our brains are very soft organs that are surrounded by spinal fluid and are protected by the hard outer covering of our skulls.
Under normal circumstances, spinal fluid cushions the brain and keeps it from crashing into the skull. However, if our heads or our bodies are hit hard, our brains can slam into our skulls and result in traumatic brain injuries (TBIs). TBIs are also caused when the skull is fractured and the brain is directly damaged by outside force.
 Although concussions, which we’ll discuss later, are sometimes referred to as mild TBIs, the reality is that no injury to the brain is mild and repeated injuries will lead to neurological degeneration that includes dementia.
Although concussions, which we’ll discuss later, are sometimes referred to as mild TBIs, the reality is that no injury to the brain is mild and repeated injuries will lead to neurological degeneration that includes dementia.
TBIs are complex neurological injuries that result in a wide variety and severity of symptoms and disabilities.
The least severe symptoms of TBIs – and these may not happen immediately and, in fact, may occur some time after the injury, can include:
The most severe symptoms of TBIs can include:
 The most common causes of TBIs, according to the Centers for Disease Control, are:
The most common causes of TBIs, according to the Centers for Disease Control, are:
In the category of TBIs from falling, most of the falls occur disproportionately in the very young (55% of falls among children occur in children between the ages of 0 and 14) and the very old (81% of falls among adults occur in adults who are 65 or older).
Most of the TBIs in the Other category (19%) are from personal firearms and military weapons.

Courtesy of Sports Legacy Institute (http://www.sportslegacy.org/)
A type of TBI that is more frequently in the headlines today is Chronic Traumatic Encephalopathy (CTE). CTE is brain damage that occurs as a result of repeated concussions (a concussion is defined as injury to the brain from a direct blow to the head or from the head or upper body being violently shaken).
The first identified variant of CTE was described in 1928 by forensic pathologist Dr. Harrison Stanford Martland as pugilistic (from the Latin word pugil, which is translated as “boxer” or “fighter”) dementia. The symptoms included tremors (Parkinsonism), slowed movement, mental confusion, and speech difficulties.
In 1973, the neuropathology of pugilistic dementia was discovered and described by a team of pathologists led by J. A. Corsellis who documented their findings after performing thorough autopsies on the brains of 15 deceased boxers.
 Former boxing heavyweight champion Muhammad Ali began boxing in Kentucky when he was 12 years old.
Former boxing heavyweight champion Muhammad Ali began boxing in Kentucky when he was 12 years old.
By the age of 18, he had boxed his way to the heavyweight gold medal at the Olympics (1960).
A few months later Ali began his professional boxing career. He quickly gained national prominence because of his skill in the ring and his trademark quote: “Float like a butterfly, sting like a bee. The hands can’t hit what the eyes can’t see.” He boxed professionally until his retirement in 1981.
In 1984, Ali was diagnosed with Parkinsonism (the tremors of pugilistic dementia) and his neurological health has deteriorated steadily to include all the advanced symptoms of  this variant of CTE.
this variant of CTE.
His wife, Lonnie, is his caregiver and contributed to a moving article that AARP published last year about what she and Ali deal with on a daily basis as a result of the neurological degeneration that CTE has caused.
CTE has increasingly become a major health concern in the high-contact sports of professional wrestling, ice hockey, soccer, and football as more and more current and retired athletes are showing symptoms consistent with CTE.
 In recent years, football – and especially professional football – has become the focal point for a closer examination of CTE. Not only has this sport become more violent in terms of how the game is played, but how concussions are treated – or not treated – has also come under greater scrutiny.
In recent years, football – and especially professional football – has become the focal point for a closer examination of CTE. Not only has this sport become more violent in terms of how the game is played, but how concussions are treated – or not treated – has also come under greater scrutiny.

Joseph Maroon, Pittsburgh Steelers Team Doctor
Although NFL team doctors assert that CTE is “rare” or “overexaggerated,” the hard scientific neurological and physiological evidence proves that these doctors are simply paid hirelings who care more about their paychecks than they do about the overall health of the players.
Let’s examine the facts. In a 2014 landmark study by the largest brain bank in the United States, 76 of the 79 brains of deceased NFL players that pathologists examined had TBI, and specifically, CTE.
A class action lawsuit has been filed – and a tentative agreement reached with the NFL – by retired NFL football players and/or their families (some of the players have already died from neurodegenerative causes) which claims that players were not (a) adequately protected from suffering concussions, (b) medically treated properly following concussions, and (c) provided adequate medical compensation to treat the burgeoning costs of CTE as it progresses.
This gist of this lawsuit is that the NFL used – and abused – these players to fabulously guild the seemingly-endless coffers of the NFL, often forcing the players by intimidation or fear to get back on the field as soon as they could after suffering a concussion (often in the same game), and then abandoned their responsibility to their former employees (as part of their contractual agreement) as soon as the employees began costing them money instead of making them money.
Even more damning to the NFL is the actuarial report accompanying the lawsuit that indicates that at least 1/3 of NFL players will suffer CTE.
If there is a silver lining in all of this, it is that the younger NFL players have a much greater awareness of the relationship – and their increased risk – between professional football and CTE.
They are aware of the very real probability that they will be one of the 1 out of every 3 players who develops CTE.
And they’re choosing their long-term health, including their brain health, over temporary fame and fortune.
 An unprecedented number of younger – and in-their-prime in the professional football world – NFL players have already retired before the 2015-2016 season begins.
An unprecedented number of younger – and in-their-prime in the professional football world – NFL players have already retired before the 2015-2016 season begins.
They include:
While Finnegan, Locker, and Worilds did not publicly cite CTE as a factor in their premature retirements from the NFL, there can be no logical reason to doubt that the mounting evidence was a factor in their decisions.
 Borland just finished his rookie season (2014-2015) with the San Francisco 49ers, but he revealed after the season that he suffered a concussion in training camp last fall. Instead of reporting the concussion, Borland covered it up so that he could continue to practice and win a starting position on the team.
Borland just finished his rookie season (2014-2015) with the San Francisco 49ers, but he revealed after the season that he suffered a concussion in training camp last fall. Instead of reporting the concussion, Borland covered it up so that he could continue to practice and win a starting position on the team.
This is the kind of competitive pressure that gets put on these young players by the NFL (yes, Borland made the decision and he bears the responsibility for it, but had he reported the concussion, he would have been replaced and lost the starting spot and may not have played all season).
Fortunately, though, Borland came to his senses and realized how much he had jeopardized – and would continue to – his neurological health.
As he said on the March 16, 2015 edition of ESPN’s Outside the Lines, “”I just thought to myself, ‘What am I doing? Is this how I’m going to live my adult life, banging my head, especially with what I’ve learned and knew about the dangers?'”
We can only hope that more athletes in high-contact sports will know the higher risks of TBIs they face, not just in the professional leagues, but at the amateur levels, and they will choose to walk away from certain neurological damage.
In the meantime, we have a better understanding just in our daily lives of how TBIs can happen and what the results can be, so I hope that we’re a little more observant and attentive after falls with our little loved ones and our older loved ones, especially those already going through the journey through dementias and Alzheimer’s Disease, as they are even more prone to falling than the general elderly population.
As Sergeant Phil Esterhaus says at the end of every roll call on Hill Street Blues (a favorite TV show of mine during my high school and college years), “Hey, let’s be careful out there.”
Our loved ones with dementias and Alzheimer’s Disease are much more susceptible to getting the flu than the general population, including senior citizens in general (the overwhelming majority of deaths from the flu each year occur in people over the age of 65).
With the peak of flu season upon us, it would be a good idea to review some basics about the flu. Click on the infographic below to see the full article.

Source: Fix.com
 This is the last in a series of posts that discusses everyday practical needs that almost no one ever talks about in providing care and making life easier for both us as caregivers and the loved ones with dementias and Alzheimer’s Disease that we care for.
This is the last in a series of posts that discusses everyday practical needs that almost no one ever talks about in providing care and making life easier for both us as caregivers and the loved ones with dementias and Alzheimer’s Disease that we care for.
In the first post in this series, we discussed how to make things easier day-to-day for our loved ones in the areas of eating and incontinence.
In the second post in this series, we discussed day-to-day helps in the areas of personal grooming and bathing in the journey through dementias and Alzheimer’s Disease with our loved ones.
In this post, we’re going to discuss the other day-to-day areas where we can make care easier for ourselves and our loved ones in the journey through dementias and Alzheimer’s Disease.
The first area we’ll look it is how to effectively and safely address limited mobility and problematic mobility issues that arise both as a result of the progression of these degenerative neurological diseases and the aging process itself.
Because dementias and Alzheimer’s Disease affect the parts of the brain that control movement and balance, even our loved ones with no other health-related mobility limitations will eventually develop a shuffling gait and maintaining their balance when standing or walking will be difficult, increasing their risk of falls and injuries.
Our loved ones will also have a much harder time getting up and down from a seated position.
One of the most noticeable difficulties will be getting up from and sitting down on the toilet.
 Many occupational therapists will recommend, as part of the home adaptive accessory purchases, buying a bedside commode for use when our loved ones are sick and unable to easily get to the bathroom or when – especially toward the end of life – if our loved ones aren’t completely immobile, walking any distance is too difficult.
Many occupational therapists will recommend, as part of the home adaptive accessory purchases, buying a bedside commode for use when our loved ones are sick and unable to easily get to the bathroom or when – especially toward the end of life – if our loved ones aren’t completely immobile, walking any distance is too difficult.
A bedside commode will cost between $30-$40 out-of-pocket and can be purchased at a local medical supply store. However, with home health care or palliative health care, this will be covered by insurance (Medicare or other insurance) as part of the home health care or palliative health care services and equipment.
Occupational therapists will also recommend using the chair portion of the bedside commode over the bathroom toilet in the interim to facility easy standing and sitting.
This is not the best option.
The bedside commode chair is wide, and often won’t fit well, especially in smaller bathrooms, and securely enough over the toilet for this application.
Additionally, the distance between it and the toilet (even with the open guard that comes with most of them) makes keeping the toilet area clean and sanitary more difficult.
So I recommend, instead, a raised toilet seat with arms.
 A raised toilet seat will cost around $60 out-of-pocket and can be purchased at a local medical supply store. However, with home health care or palliative health care, this may also be covered by insurance (Medicare or other insurance) as part of the home health care or palliative health care services and equipment.
A raised toilet seat will cost around $60 out-of-pocket and can be purchased at a local medical supply store. However, with home health care or palliative health care, this may also be covered by insurance (Medicare or other insurance) as part of the home health care or palliative health care services and equipment.
The advantage of a raised toilet seat with arms is that it attaches to the toilet, is more secure when standing and sitting, and is more comfortable than the bedside commode chair. It is also more sanitary and easier to keep clean.
Installation is quick and easy. With the toilet seat up, the raised toilet seat is placed directly on the bowl of the toilet where it attaches securely with a large plastic bolt to the inside of the bowl.
As our loved ones progress in their journeys through dementias and Alzheimer’s Disease, they will become more sedentary than active.
This will mean sitting for long periods of time. Motor skills become more muted with neurological degeneration and a lot of the automatic sensory information that the brain gets, processes, and responds to will disappear.
Therefore, it will become less automatic for our loved ones with dementias and Alzheimer’s Disease to feel the natural discomfort of sitting in one position or sitting still for a long period of time that, when we’re neurologically healthy, causes us to automatically move and shift weight frequently when we’re seated.
This results in the increased likelihood of pressure sores and pressure ulcers developing. Once the skin breaks down in this manner, treatment and healing are difficult at best. Because of this, infection and sepsis often follow leading to death.
The most effective way to prevent pressure sores and pressure ulcers from sitting for long periods of time is to buy padding for 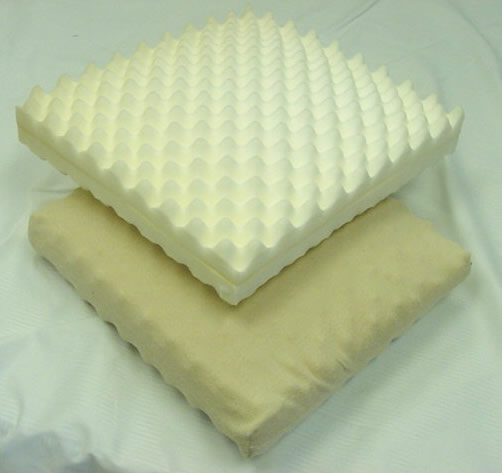 the chair that distributes weight more evenly and that does the work of ensuring that automatic shifting of weight occurs.
the chair that distributes weight more evenly and that does the work of ensuring that automatic shifting of weight occurs.
The least expensive way (about $20) to do this is to put a thick (at least 4″) egg-crate-type foam pad (most come with a plastic covering to help with incontinence issues) in the chair that our loved ones with dementias and Alzheimer’s Disease spend most of their seated time in.
These can be purchased at most big-box retail stores.
Another physiological change that occurs for our loved ones as dementias and Alzheimer’s Disease progress is difficulty swallowing (known as dysphagia). This difficulty includes liquids and solid foods, as well as medication.
Dysphagia presents two real dangers to our loved ones. One is choking. The other is aspirating food into the lungs, which can lead to the development of pneumonia. In fact, it is more common than not that pneumonia is the cause of death for our loved ones with dementias and Alzheimer’s Disease.
That’s how serious swallowing issues are for our loved ones.
However, we can help mitigate this risk by some very simple techniques that will facilitate easier swallowing and reduce the risks of choking and aspirating food into the lungs.
Let’s start with taking medication since this is usually where swallowing issues appear first in the journey through these neurological diseases.
However, before I discuss the technique that usually is helpful for our loved ones to more easily swallow medications, it is important to discuss the medications themselves and the form they are administered in.
 First, as caregivers, we should all have a pill cutter (also known as a pill splitter) as part of pharmacy stash. These can be pick up at any pharmacy very inexpensively.
First, as caregivers, we should all have a pill cutter (also known as a pill splitter) as part of pharmacy stash. These can be pick up at any pharmacy very inexpensively.
This will come in handy when managing medications with varying dosages (such as diuretics or glucocorticoids like prednisone, which might be increased temporarily or gradually and then decreased the same way).
However, I strongly advise against a pill crusher and crushing any medications (although assisted living facilities and nursing homes routinely ignore this when administering medications to residents with dysphagia). The reason is because there are medications that when crushed can cause serious side effects and become completely non-therapeutic.
 When our loved ones with dementias and Alzheimer’s Disease begin to have problems swallowing medications with water or juice, the easiest and usually-most-effective way to help them be able to swallow the medication is to use applesauce (I recommend unsweetened).
When our loved ones with dementias and Alzheimer’s Disease begin to have problems swallowing medications with water or juice, the easiest and usually-most-effective way to help them be able to swallow the medication is to use applesauce (I recommend unsweetened).
Put the pill on about 2/3 teaspoon of applesauce, which goes down the throat more easily, and swallowing should be much easier.
If our loved ones have medication that come in a large pill form (potassium supplements are a good example and because they tend to dissolve in the mouth and are very bitter are not a good candidate for cutting in half), we should have our loved ones’ primary care providers (PCPs) prescribe a different form of the medication.
Some medications are available in a liquid form (potassium, for example, comes in a liquid form and can be mixed with applesauce).
Other medications are available in a sprinkle form (for example, Depakote, which is often used for mood balance in Lewy Body dementia because of the high sensitivity to anti-psychotics like SeroquelXR, is available in sprinkle form and can be mixed with food).
If a liquid or sprinkle form of the medication is not available, then we should work with the PCP to change to a smaller-pill alternative that will produce equivalent results.
As swallowing becomes even more difficult for our loved ones, liquids and solid food may need to be altered as well.
Sometimes this can be as simple as cutting up food (meat, for example, can be very hard to chew thoroughly in large pieces) into very small pieces and modifying or eliminating foods.
Easy foods to modify are vegetables. Raw vegetables and salads become difficult to chew and swallow for our loved ones as they reach this stage of dementias and Alzheimer’s Disease. Easy alternatives to ensure good nutrition are cooked beans and finely chopped vegetables, including  some of the lettuces we normally use for raw salads (avoid kale and mustard greens – I use these for raw salads – because even cooked, they can be difficult to swallow).
some of the lettuces we normally use for raw salads (avoid kale and mustard greens – I use these for raw salads – because even cooked, they can be difficult to swallow).
You can also use these cooked beans and vegetables to make a creamy pureed soup. The key is to make the soup so that it approximates the texture of applesauce (not too thick and not too thin).
And I will pass this modification on as a personal note – if you want my recipe, email me at goinggentleintothatgoodnight@gmail.com – for cornbread. Crumbly, grainy, and textured breads and crackers are eliminated from our loved ones’ diets when swallowing everything becomes problematic. The reason is that they can choke and aspirate the little grains and crumbs into their lungs.
But my mama loved cornbread and I wanted to see if I could find a way to keep it in her diet. I had been doing some reading on healthy substitutions in baking (for oil, for sugar) prior to this ever being an issue, so I decided to try one of the healthy substitutions for oil – yogurt – in a batch of cornbread to see if it would change the texture from grainy to smooth. It worked perfectly (beautiful texture) and we were able to keep that in Mama’s diet (and any time we can find a way to do this, please go for it and try it!).
Swallowing issues may advance to the point where the dysphagia diet levels need to be implemented. There are three levels in this diet, depending on badly swallowing is compromised. I have not personally used these, although I’m familiar with them.
However, this is something that a speech therapist with home health care or palliative health care is qualified to and can help and guide us through at this juncture with our loved ones with dementias and Alzheimer’s Disease.
I can’t emphasize enough how important it is for us as caregivers to have one or other of home health care or palliative health care on board as we provide care for our loved ones since they have resources, like speech therapists, who are available to walk us step-by-step through each phase or issue that we may encountered.
This is the last post in this series. If there are other day-to-day “in-the-moment” things related to caregiving for our loved ones with dementias and Alzheimer’s Disease that would make your life – and, no doubt, many others’ – easier that you would like to see discussed, leave a comment here and I’ll work with you to get you the answers and the help you need.
And please don’t forget to share this on social media. Dementias are more prevalent than ever – and will only increase from this point on – and more and more people are in the role of caregiving for their loved ones.
I often have people ask me what they can do to help and support other caregivers. All you have to do is share. I’ll do the hard lifting of research and writing. 🙂
Even if you don’t know all the people in your online networks, by sharing this information with them, you may be giving a lifeline to someone who is struggling, feeling overwhelmed, and completely alone on their journey.
We never know whose lives are crossing the path with ours. And this may be a random act of kindness that you’ll never even know you did. All you have to do it hit the Share buttons (and there is an email button for those who may not be on social media) for the social media forums you’re on to pass this information along to whoever may need it and can use it.
Thanks!
 Exercise and fitness are important aspects of life and are beneficial for everyone, but particularly for our loved ones with Alzheimer’s Disease and dementias.
Exercise and fitness are important aspects of life and are beneficial for everyone, but particularly for our loved ones with Alzheimer’s Disease and dementias.
There has been significant research that shows that leading a life that is physically active and includes regular exercise can have a positive impact on overall health and well-being.
People who exercise regularly have improved levels of general cardiovascular health, stronger bones and, therefore, a reduced risk of osteoporosis. They also tend to sleep better at night and have improved strength and balance, which can reduce the fall risks for our loved ones with dementias and Alzheimer’s Disease.
Exercise has other wonderful health benefits too. Any level of regular physical exercise can have a positive impact on emotional health.
Exercise may help alleviate some of the symptoms of depression, a common condition in our loved ones with dementias and Alzheimer’s Disease, particularly in the early steps of the journey through these diseases.
Exercise can be beneficial with depression symptoms because it releases endorphins and other mood-enhancing brain chemicals. And even if our loved ones have reduced mobility or are in the middle-to-late steps of the journey through dementias and Alzheimer’s Disease, there are still ways to incorporate regular exercise into their daily routines.
Listed below are a few simple exercises for our loved ones with dementias and Alzheimer’s Disease.
Exercises Using A Chair
Seated exercises are ideal for our loved ones with dementias and Alzheimer’s Disease since they tend to have stability issues. Additionally, chair exercises are a great way to begin getting more physically active if our loved ones haven’t been for a while.
Seated exercises can help to build and maintain essential muscle strength and balance, but they are much less strenuous than standing exercises and reduce the risk of falls and/or injuries.
It’s important to use a sturdy chair with a back (I would recommend one that’s roomy with arms to prevent our loved ones from falling off sideways) for seated exercises and for us to be close by to assist if need be.
With our loved ones with dementias and Alzheimer’s Disease, it’s important to take the time to do these exercises at their pace. This includes taking the extra time to patiently coach – without expecting perfection in execution or repetition, with “good enough” done safely being “great.”
It would be ideal to begin each exercise session by breathing in as deeply as possible and then breathing out gently (if our loved ones are able to lift their arms to the side while doing this, it will help increase lung capacity, but if not, that’s okay).
We may have to coach and show our loved ones how to do this, doing the breathing exercises with them to encourage them to follow our example. Repeat this up to a maximum of ten times.
1st exercise (shoulder rolls): Lift the left shoulder up, then take a deep breath in. Breathe out as the shoulder drops. Then, lift the right shoulder up, then take a deep breath in. Breathe out as the shoulder drops. Alternate between the left and right shoulder up to ten times.
2nd exercise (neck strength): In the same sitting position, tilt the head back. Following the same breathing pattern as before, breathe in as the head is tilted back, then breathe out the head moves forward. Then, breath in as the head is turned to the left and breath out as the head is turned to the right. Repeat, alternating between back and forth and left and right up to ten times.
3rd exercise (sitting march): Pace can be as slow or fast as is comfortable. Lift the right knee up and breathe in; put that same foot down and breathe out. Repeat the same process with your left leg. Alternate between left leg and right leg up to twenty times.
4th exercise (leg stretches): Extend the left leg fully, breathing in as it’s extended, and breathing out as it is bent. Repeat with right leg. Alternate between left and right legs up to ten times.
5th exercise (ankles): Cross the left leg over the right leg, and rotate the left foot. Then, cross the right leg over the left leg, and rotate the right foot. Alternate between left and right foot, breathing rhythmically throughout, up to ten times.
Exercising to Music
In the early steps of the journey through dementias and Alzheimer’s Disease, our loved ones may be able to do slightly more strenuous exercises around the home, such as gardening, walking up and down the stairs or even dancing.
Exercising to music can make the activity a much more enjoyable experience. Since listening to music can also be beneficial in many ways for our loved ones with dementias and Alzheimer’s Disease, incorporating music into daily activities like exercise makes perfect sense in our overall care strategy.
![]()
 This is the second in a series of posts that discusses everyday practical needs that almost no one ever talks about in providing care and making life easier for both us as caregivers and the loved ones with dementias and Alzheimer’s Disease that we care for.
This is the second in a series of posts that discusses everyday practical needs that almost no one ever talks about in providing care and making life easier for both us as caregivers and the loved ones with dementias and Alzheimer’s Disease that we care for.
In the first post in this series, we looked at how to make things easier day-to-day for our loved ones in the areas of eating and incontinence.
In this post, we’ll look at the areas of personal grooming and bathing in the journey through dementias and Alzheimer’s Disease with our loved ones.
The progressive neurological damage of these diseases can affect our loved ones in several ways in the areas of bathing and personal grooming, which may necessitate accommodations for them in these areas.
Before we discuss those in detail, it is imperative that we always respect the dignity of our loved ones with dementias and Alzheimer’s Disease, and that we give them as much autonomy and independence in all areas of their lives, including these, as is safe.
Dignity is not negotiable. Our loved ones deserve that at all times and we owe them that at all times. Being more dependent and less able to take care of themselves is hard enough on our loved ones, but to not respect and maintain their dignity is humiliating and devastating.
Our loved ones with dementias and Alzheimer’s Disease have been and are being robbed of their quality of life by an unseen or several unseen thieves in their brains. We should not be adding insult to injury by robbing them of their dignity.
Independence is also critical to the well-being of our loved ones. Safety concerns will, at times, limit full independence. However, that should be the only reason we curtail independence in any way.
Being a lot slower at doing things, being less than perfect at doing things, or forgetting how to do something but trying anyway should never be reasons why we take independence away from our loved ones. If we do, shame on us.
The requirements of making bathing – including washing hair -easier for our loved ones with dementias and Alzheimer’s Disease will change as these neurological diseases progress.
However, there are several things that we should be aware of throughout the course of these diseases:
Showering or a full bath every day is hard on and can damage the fragile skin of our elderly loved ones. A good rule of thumb is alternating showering or full bathing every other day with the equivalent of a sponge bath.
Harsh soaps and shampoos will also damage skin, including the scalp. Baby bath wash and baby shampoo is the gentlest option for bathing and shampooing hair.
Skin also dries out as our loved ones age – diuretics will make skin dryness even worse – so we should make sure our loved ones are lotioned up well each day with a good hydrating lotion.
Bathtubs for older folks are difficult to get in and out of and present a greater danger of falls.
If you are reading this with younger loved ones you may be caring for in the future or even with yourself in mind, please make sure that a first-floor bathroom has a walk-in shower (ceramic or fiberglass frame – a metal frame can cut), which can be adapted for even greater safety using assistive devices.
When staying in a hotel, be sure to request a handicapped room since these have walk-in showers (which are even wheelchair accessible, if needed).
Make sure the bathing area is the warmest room in the house. As our loved ones get older and as dementias and Alzheimer’s Disease progress, sensitivity to cold is even more pronounced.
If there is no additional heater built into the bathroom, use a space heater. About 15 minutes before bathing time, turn the heater on and close the door. This will ensure that the bathroom is at a comfortable temperature by bath time.
Have everything you need for bathing, personal grooming, and dressing ready before starting the bathing process.
This makes the process go more smoothly and efficiently and it ensures that we don’t have to leave our loved ones unattended – with the possibility of falls and/or injury – during the process.
Water temperature is crucial and we must ensure that it’s not too hot or too cold. Run the shower (or sponge bath water) until it is on the warmer side of lukewarm as a general guideline.
The sensation of water pouring down from a shower can sometimes be frightening for our loved ones with dementias and Alzheimer’s Disease as they approach the middle and late steps of these diseases.
My personal theory is that it’s a combination of three things: a heightened sensitivity to change (resulting in confusion and anxiety), the suddenness of it, and the feeling of being wet.
We will notice that some days showering is not an issue and other days it’s a huge issue.
On the days that it’s a huge issue, it’s important that we don’t force our loved ones into a situation that is frightening for them, because this will increase fear, anxiety, confusion, and disruptive behavior.
Instead, we should opt for a sponge bath or cleanup with adult washcloths and try again another day.
 As far as bathing and shampoo products go for shower days, I recommend Johnson’s Moisture Baby Wash and Johnson’s Baby Shampoo.
As far as bathing and shampoo products go for shower days, I recommend Johnson’s Moisture Baby Wash and Johnson’s Baby Shampoo.
While there are generic brands of baby body washes and baby shampoos, I found the quality inferior (i.e., they were more watered down) to Johnson’s baby products.
 Since these are designed for delicate skin, they meet the bathing and the shampooing needs of our older loved ones with dementias and Alzheimer’s Disease as well.
Since these are designed for delicate skin, they meet the bathing and the shampooing needs of our older loved ones with dementias and Alzheimer’s Disease as well.
Additionally, the shampoo won’t irritate the eyes if it drips into them. Since following directions – such as keeping eyes closed – is harder for our loved ones to do or sustain if they are able to do it, this ensures that no harsh chemicals get into their eyes while washing their hair.
 For non-shower days, I recommend using disposable adult washcloths. Adult washcloths are large and premoistened, usually with aloe added, and can be used very effectively to clean up. They are not flushable.
For non-shower days, I recommend using disposable adult washcloths. Adult washcloths are large and premoistened, usually with aloe added, and can be used very effectively to clean up. They are not flushable.
Adult washcloths can be bought inexpensively in bulk at warehouse clubs like Sam’s Club, Costco, and BJ’s (online or in-store).
A product that many hospitals use for bathing that I do not recommend is no-rinse body wash/shampoo. One reason I don’t recommend no-rinse body wash/shampoo is that I don’t find that it does a good job of cleaning and it leaves a slight residue on skin and hair. The other reason I don’t recommend no-rinse body wash/shampoo is that it dries the skin and hair out, which makes the fragile skins of our elderly loved ones with dementias and Alzheimer’s Disease even more dry and fragile.
There are several things that we’ll need to do to ensure the bathroom and shower is safe to prevent falls for our loved ones.
Most modern bathroom floors are either ceramic tile or linoleum. Both of these surfaces are very slippery when they’re wet, so we want to ensure that the floor has an adequate amount of non-skid covering to ensure the safety of our loved ones when they are wet.
 Rugs and oversized bath mats are the easiest and least expensive way to cover the bathroom floor adequately. It’s also easy and inexpensive to ensure that they are non-skid by applying non-skid tape to the back of the rugs or bath mats. The best product I found for this is Duck® Brand Hold-It for Rugs™, which can be purchased through many venues online or at home supply stores.
Rugs and oversized bath mats are the easiest and least expensive way to cover the bathroom floor adequately. It’s also easy and inexpensive to ensure that they are non-skid by applying non-skid tape to the back of the rugs or bath mats. The best product I found for this is Duck® Brand Hold-It for Rugs™, which can be purchased through many venues online or at home supply stores.
Non-slip tub/shower mats with suction cups are the usual recommendation to keep our loved ones with dementias and Alzheimer’s Disease from slipping and falling in the shower. However, my personal experience with these is that with most shower floors, the suction cups don’t adhere well and the mat moves around easily.
 So I don’t recommend these for the shower floor. Instead, I recommend non-skid strips or tape designed specifically for the shower.
So I don’t recommend these for the shower floor. Instead, I recommend non-skid strips or tape designed specifically for the shower.
The entire floor of the shower does not need to be covered nor do the strips or pieces of tape have to be right up against each other (gaps between them are fine as long as they are not wide enough to cause a slip or fall) , but you do want the primary walking surface to have enough skid-resistant strips or tape in place to ensure safety.
Like the non-skid tape for the rugs, this is very inexpensive and provides the maximum safety for our loved ones and can be purchased online at Koffler Sales Company. There is no quality difference between the 3M™ and KSC brands, but because 3M™ is a more-recognizable brand, the price for their products is higher.
As far as the safety of our loved ones with dementias and Alzheimer’s Disease goes in the shower itself, there are two additions that I would highly recommend.
One addition is a safety grab bar. There are two kinds of grab bars for showers on the market. One kind requires no hardware to install it because it uses a suction-cup locking system. The other kind requires hardware to install it (and, if you’re not handy, may require a professional to install it).
 Although the easy-to-install grab bar is less expensive overall, I don’t recommend it for our loved ones with dementias and Alzheimer’s Disease. Because it uses a suction cup to hold it to the shower wall, with enough weight or time, it could become detached and cause a fall.
Although the easy-to-install grab bar is less expensive overall, I don’t recommend it for our loved ones with dementias and Alzheimer’s Disease. Because it uses a suction cup to hold it to the shower wall, with enough weight or time, it could become detached and cause a fall.
Therefore, I recommend the grab bar that uses hardware to attach it to the shower wall.
Although this presents work and a possible upfront cost for installation, it gives our loved ones the extra measure of safety for fall prevention.
 The other addition that I recommend is a portable shower chair.
The other addition that I recommend is a portable shower chair.
Built-in shower seats are often small and in one corner of the shower, which doesn’t facilitate easy showering.
However, the main concern with built-in shower seats for our loved ones is that they are slippery and the fall/injury potential is great.
Shower chairs allow our loved ones with dementias and Alzheimer’s Disease to sit either during the shower or when they get tired during the shower.
For the most comfort, I recommend a shower chair with a back and without arms.
The shower chair should be placed in the shower near the grab bar.
We should be on hand while our loved ones are sitting in the chair and we should always assist them – directing them to use the grab bar to help – getting up and down out of the chair. While the shower chair’s feet have rubber grips, the chair will move when our loved ones are standing up or sitting down.
In the next post in this series, we will look at how to make life easier in the areas of mobility and functionality/accessibility for our loved ones with dementias and Alzheimer’s.
 In this last installment of chapter excerpts from the book You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease, we look at the last step in the journey through dementias and Alzheimer’s Disease.
In this last installment of chapter excerpts from the book You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease, we look at the last step in the journey through dementias and Alzheimer’s Disease.
This post includes an excerpt from chapter 15, which gives comprehensive information on how to walk the last step in the journey through dementias and Alzheimer’s Disease, which is the one that we’ll take alone without our loved ones: grief.
There is no right or wrong way to grieve. There is no time limit on grief. Grief is a process and the reality is that there will always be a hole in your heart when you lose a loved one.
Grief is also complex and complicated. We not only grieve for the loss of our loved ones, but we also grieve for all that intertwined their lives with ours because we recognize that part of our lives is over in this life.
And part of the grief process is sorting through those intertwined lives, the good, the bad, the ugly, as we reflect deeply on our time together.
Some people are able to stuff the hole of loss with busyness and lots of people and lots of things and it seems like they just picked up and moved on without blinking. They didn’t, but it looks that way.
Other people move through the process of scabbing the wound of the hole of loss more slowly, in spurts and stages that at times seem interminable and like they will never end. But it does and eventually, they find a way to move on as well.
You will find that the grieving process will tell you a lot about the people who are around you in your life.
And because death and grief necessitate one of life’s major reset phases, which includes a period of purging (not all on our part) – usually for the better, although it’s incredibly painful at the time – part of that reset phase extends to the people who are around us in our lives.
We find out who the people around us are and what we mean to them during this period.
And, although it may be sad and surprising, depending on our temperaments and personalities, many of those people will exit your life if you don’t meet their expectations and time limits on what acceptable grief looks like.
We have to accept that they were never there for the long haul to begin with.
A very small group of a few other people will hang in there with you every step of the way and beyond.
That’s your inner circle. Love them. Cherish them. And do the same and more for them as life happens to them. They’re not going anywhere. You’re not either.
This series begins with the forward to the book and an explanation of why I wrote this book and why you should read it.
The series continues with the inclusion of excerpts from Chapter 1, Chapter 2, Chapter 3, Chapter 4, Chapter 5, Chapter 6, Chapter 7, Chapter 8, Chapter 9, Chapter 10, Chapter 11, Chapter 12, Chapter 13, Chapter 14, and, with this post, Chapter 15.
The steps in the journey through dementias and Alzheimer’s Disease are presented sequentially in the order in which they actually appear in the course of these neurological diseases.
There are no other books that literally walk through each step in sequential order as they emerge in the journey through dementias and Alzheimer’s Disease.
Additionally, there is no other book that discusses:
These are the things that make You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease unique and stand alone in the plethora of books about dementias and Alzheimer’s Disease.
![]()
Excerpt “Chapter 15: ‘I Have a Lock of Hair and One-Half of My Heart’”
“Death and its aftermath is the last step of this journey through dementias and Alzheimer’s Disease and it is a step that we take without our loved ones.
It is often said that in these neurological and fatal diseases that we experience death twice. The first death is the loss of the loved ones we knew before these diseases. The second death is when our loved ones take their last breath.
If hospice is on board, the first phone call we make is to them. A nurse will come out and confirm death. Hospice will also contact the funeral home and will prepare the body for transport. This includes cleaning and dressing (I actually helped our hospice nurse with this).
When the people from the funeral home get there, they will make an appointment to come in and make burial arrangements (usually the next day) and they will take the body to the funeral home and start the embalming process.
Once the funeral home people leave, the hospice nurse will collect and destroy any remaining medications and there will be paperwork to sign both to confirm the medication disposal and to end hospice services.
It’s a flurry of activity that lasts several hours, and I personally found that to be just what I needed because the reality that Mom was gone was still sinking in.“
In this fifteenth installment of chapter excerpts from the book You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease, we look at the fourteenth step in the journey through dementias and Alzheimer’s Disease.
This post includes an excerpt from chapter 14, which gives comprehensive information on how to acknowledge, recognize, and respond to the fourteenth step in the journey through dementias and Alzheimer’s Disease: the end of life and death.
As we near the end of the journey we’ve shared with our love ones, this is the last step we will take with them. This chapter talks comprehensively about how to do that with love, with gentleness, and with kindness.
This series begins with the forward to the book and an explanation of why I wrote this book and why you should read it.
The series continues with the inclusion of excerpts from Chapter 1, Chapter 2, Chapter 3, Chapter 4, Chapter 5, Chapter 6, Chapter 7, Chapter 8, Chapter 9, Chapter 10, Chapter 11, Chapter 12, Chapter 13, and, with this post, Chapter 14.
The steps in the journey through dementias and Alzheimer’s Disease are presented sequentially in the order in which they actually appear in the course of these neurological diseases.
There are no other books that literally walk through each step in sequential order as they emerge in the journey through dementias and Alzheimer’s Disease.
Additionally, there is no other book that discusses:
These are the things that make You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease unique and stand alone in the plethora of books about dementias and Alzheimer’s Disease.
![]()
Excerpt “Chapter 14: ‘As the Final Curtain Falls Before My Eyes’”
“This step is the next to the last step in the journey that our loved ones with dementias and Alzheimer’s Disease take. It can be a lengthy step of months or a short step of weeks or a shorter step of just a few days. Regardless of the amount of time, though, this step is harder, I believe, on us than it is on our loved ones.
This step is a two-process step: the body begins shutting down in the first process and active dying occurs in the second process.
One of the first signs that the body is beginning to shut down that we’ll see with our loved ones with dementias and Alzheimer’s Disease is that they will start sleeping a lot more.
This usually begins a few months before death occurs. Often, this is a pattern of an hour or two of wakefulness followed by naps and dozing on and off during the day, with fatigue setting in early in the evening and a full night’s sleep ensuing.
In short, our loved ones will be asleep more than they are awake.
Another sign may be a decreased desire for food and drink. It is important to not to try to force food and liquids on our loved ones with dementias and Alzheimer’s Disease if they don’t want them. As the body starts its elaborate shutdown process, there simply isn’t a need for much nourishment. Additionally, because our loved ones are not very active, they don’t burn a lot of calories nor do they need as much sustenance.
However, what is also likely to happen is that our loved ones will want or need nourishment at odd times of the day (not necessarily a normal meal time), and when they do, try to keep food and drinks healthy and light (easy to digest).
Often, during this time of shutting down, our loved ones with dementias and Alzheimer’s Disease will, when they are awake, both sort through their lives and work to make peace with anything in their pasts that they believe is left unsettled.“
In this fourteenth installment of chapter excerpts from the book You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease, we look at the thirteenth step in the journey through dementias and Alzheimer’s Disease.
This post includes an excerpt from chapter 13, which gives comprehensive information on how to acknowledge, recognize, and respond to the thirteenth step in the journey through dementias and Alzheimer’s Disease: ensuring that our loved ones always know that we love them and are committed to them all the way.
Although showing our love and commitment is something we do throughout our lives with our loved ones, this step is another conscious one that we need to practice as these neurological diseases progress and our loved ones seem to begin to disappear and we can bogged down as their care needs increase. There is never not enough time for love.
This series begins with the forward to the book and an explanation of why I wrote this book and why you should read it.
The series continues with the inclusion of excerpts from Chapter 1, Chapter 2, Chapter 3, Chapter 4, Chapter 5, Chapter 6, Chapter 7, Chapter 8, Chapter 9, Chapter 10, Chapter 11, Chapter 12, and, with this post, Chapter 13.
The steps in the journey through dementias and Alzheimer’s Disease are presented sequentially in the order in which they actually appear in the course of these neurological diseases.
There are no other books that literally walk through each step in sequential order as they emerge in the journey through dementias and Alzheimer’s Disease.
Additionally, there is no other book that discusses:
These are the things that make You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease unique and stand alone in the plethora of books about dementias and Alzheimer’s Disease.
![]()
Excerpt “Chapter 13: ‘And Know They Love You’”
“At this step, and indeed throughout the entire journey of dementias and Alzheimer’s Disease, we must always make sure that our loved ones know the we love them, we care about them, and we are committed to them.
As our loved ones become more dependent on us and as they lose cognition and neurological function, they often become fearful. Their fears include being isolated, being abandoned, being a burden, and being in the way. For those who are still able to communicate at this step, much of their conversations with us will include these fears.
It is our job to allay those fears and remind our loved ones with dementias and Alzheimer’s Disease that we’re on their side and we’re not going anywhere. Spending a lot of time with them becomes more critical at this step as do what we do with our loved ones during that time together.
How can we demonstrate our love, our commitment, our care and our concern in tangible ways?
One of the most reassuring things that we can do for our loved ones with dementias and Alzheimer’s Disease is to spend quality time with them. This is not just spending time, but it is time where our attention is completely dedicated to them.
While quality time can include some sort of fun or interesting activities, more often than not, it is just being with them and listening to them, interacting with them, and giving them our undivided attention.”
In this thirteenth installment of chapter excerpts from the book You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease, we look at the twelfth step in the journey through dementias and Alzheimer’s Disease.
This post includes an excerpt from chapter 12, which gives comprehensive information on how to acknowledge, recognize, and respond to the twelfth step in the journey through dementias and Alzheimer’s Disease: maintaining the dignity and as much independence as is safe for our loved ones as they become more dependent on us.
This is so critical – and, unfortunately, often overlooked or forgotten – that it must be recognized as a conscious step that we as caregivers must take and must always remember as we go through this journey with our loved ones.
This series begins with the forward to the book and an explanation of why I wrote this book and why you should read it.
The series continues with the inclusion of excerpts from Chapter 1, Chapter 2, Chapter 3, Chapter 4, Chapter 5, Chapter 6, Chapter 7, Chapter 8, Chapter 9, Chapter 10, Chapter 11, and, with this post, Chapter 12.
The steps in the journey through dementias and Alzheimer’s Disease are presented sequentially in the order in which they actually appear in the course of these neurological diseases.
There are no other books that literally walk through each step in sequential order as they emerge in the journey through dementias and Alzheimer’s Disease.
Additionally, there is no other book that discusses:
These are the things that make You Oughta Know: Acknowledging, Recognizing, and Responding to the Steps in the Journey Through Dementias and Alzheimer’s Disease unique and stand alone in the plethora of books about dementias and Alzheimer’s Disease.
![]()
Excerpt “Chapter 12: ‘Help Me Live With Dignity ‘Til the End’”
“As our loved ones with dementias and Alzheimer’s Disease progress through their journeys, they reach this step where their dignity and their independence could be compromised. It is our job to ensure that we preserve their dignity to the end and ensure as much independence as is safe to the end.
Dignity is something that all human beings should have until they take their last breath. This includes respect and honor toward them, no matter what circumstances they may find themselves in. It is no different for our loved ones with dementias and Alzheimer’s Disease.
In addition to dignity, it is also important for us to ensure that our loved ones have as much independence – guaranteeing safety at all times – over their own bodies and their own care as they are able to handle.
It will take them longer and everything may not be perfect, but as long as our loved ones with dementias and Alzheimer’s Disease can participate in their care, their lives, and our lives safely, the more happy and satisfied they will be and the more dignity and honor we will be showing them.
What does this look like in practice?
Incontinence and toileting
When our loved ones reach this step, we may begin to have to help them with toileting. Generally, urinary incontinence is the first toileting issue we encounter. This may be due more to age and medication than the actual loss of urinary continence, so our loved ones will likely know they need to urinate, but just not be able to make it in time.
We want the transition to adult incontinence clothing to be as easy and stigma-free for them as possible, so we should treat the clothing, accidents, and any other issues we encounter with no fuss and calmly and normally.”
