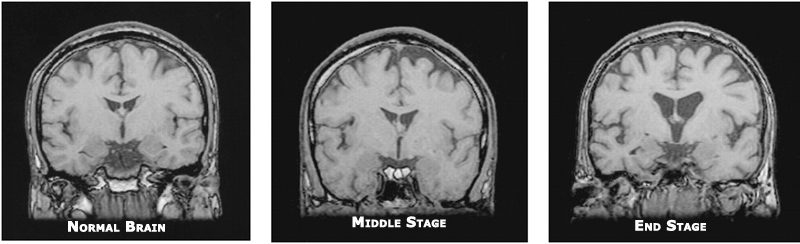
Kay Bransford and I seem to be on the same page a lot these days, but I see that we seem to be the only ones willing to tackle these subjects, so I guess we will keep sounding the drums that all of us need to be preparing in advance for the possibility that something – whether it’s Alzheimer’s Disease, dementias, other life-threatening illnesses, or simply time and chance – could suddenly and dramatically or slowly and insidiously render us incapable of taking care of our own affairs.
It seems to me that the very thing we try most to avoid thinking about, talking about, planning for is the very thing that will eventually happen to us all. And that is death.
Denial is, in my opinion, stronger and more pervasive in this area of life than in any other. “If I don’t think about it, then it isn’t real” seems to be the underlying thinking of this denial. I’m here to tell you that all the denial in the world won’t take away its inevitability of happening.
None of us, except those who chose to usurp God’s will and end their own lives, know how or when we’re going to die.
I believe most of us assume it will be quick and instantaneously, but the reality is that, in all likelihood, most of us will probably have a period of decline in which we will need help handling our financial, legal, and medical affairs before we take our last breaths.
And, after we take our last breaths, someone will have to take care of getting us buried and ending our financial, legal, and medical status among the living.
Who would that be for you? Yes, you, the one who is reading this post. Do you know? Does that person know? If that person knows, have you made this as easy as possible for him or her by doing your part and making sure he or she has everything he or she needs to do what needs to be done?
Or, because you don’t want to think about it or talk about, will that person have the burdensome responsibility of trying to figure it out all on his or her own?
We say we don’t want to be burdens to our loved ones. By taking care of this, you and I – we – have taken a big step toward easing the magnitude of that burden that, if we live long enough, will be shouldered by our loved ones.
I did my first will and living will shortly after I turned 21. I had just graduated from college, but not before having a very serious car accident (one that I miraculously survived with some significant injuries, but nothing like what I should have suffered) just before I graduated.
I’d never been that close to being face-to-face with death before, but it made me realize that I needed to make sure that my affairs – and they were paltry in those days but even then I had life insurance – were in order for the ones I’d leave behind.
From that point on, I have been meticulous about keeping my will up-to-date, the beneficiaries on my insurance policies up-to-date, and all the information my executor will need to take care of things up-to-date. I added a DNR to my medical wishes about 20 years ago, I got my cemetery plot 15 years ago, and I wrote out my funeral service and burial wishes about 10 years ago.
Additionally, my executor has updated access and account information to everything online and offline to finish up my earthly affairs when I’m gone.
 This, in my opinion, is the last act of kindness I can do in this physical life. It is also one of the greatest.
This, in my opinion, is the last act of kindness I can do in this physical life. It is also one of the greatest.
Mama used to worry that something would happen to me (i.e., that I would die before she did) and then about what would happen to her. There were times in our lives together that could have been a possibility, but I always reassured her that I’d be there with her to the end. And I was by the grace of God.
Of my parents, Daddy was a paradox when it came to this subject. On the one hand, he had life insurance that would take care of Mama after his death and he insisted, in the year before his death, that Mama get her own checking and savings accounts and get credit cards in her name only.
On the other hand, there were other areas in which he had great difficulty facing his mortality. I remember Mama suggesting that they start getting rid of clothes and other things they weren’t wearing or using anymore and Daddy’s response: “the girls can take care of that.”
The will that Daddy had in effect, until shortly before his death, was the one that he had drawn up just after he and Mama adopted us. None of the information was pertinent or relevant anymore.
After much and extended (I’m talking a couple of years) discussion between Mama and him, they finally went to a lawyer, about six weeks before he died, to have a current will drawn up.
Mama was just the opposite. Somehow, I think all the deaths of close and beloved relatives in her early years made the inevitability of death more real to her. She, primarily, during our growing up years, talked on a regular basis about what would happen to us if she and Daddy died and how we needed to take care of each other and be good kids so the road without them would be easier for us.
Not long after Daddy died, she and I sat down together (I was now checking in daily and helping her navigate through some of the things that Daddy had done and offering advice and assistance as she needed it) and she told me what she wanted – and didn’t want – as far as end-of-life wishes.
We went to an attorney together and she did a will (which she later changed to a revocable living trust), living will, and all the POA paperwork. I had copies, she had copies, and she put copies in a safety deposit box at the bank.
At that time, I didn’t need or want knowledge or access to her financial accounts, but as time went on, she needed more of my help in dealing with them, so she gave me access to get into the accounts and help her (we always sat down and did this together until she wasn’t able to anymore) keep up with bills and what she had.
By doing this with me, Mama made things much easier for me when the time came that I had to step in because she couldn’t do it.
I can’t thank Mama enough for her foresight with this gift. Instead of having to focus on everything brand new coming at me at once, I could focus on what was most important, and that was Mama: loving her, caring for her, being there for her.
The last couple of months Mama was alive, we’d be sitting close, holding hands, and talking and suddenly she’d say “I don’t want be a burden on you,” with tears rolling down her cheeks. I’d squeeze her hands and pull her closer in a hug, kissing the tears away from her cheeks, saying, “Mama, you’re not a burden to me. I love you unconditionally. I wouldn’t be anywhere else doing anything else but right here doing this with you.”
Mama would relax in my embrace and I would hold her tighter as I said these words because they were true and we both recognized that they were true, but most of all, I recognized how easy Mama had made things for me by equipping me with what I needed to step in easily and take care of the routine things so that I could save my energy, my focus, and my love for taking care of her.