 In my book review of The End of Absence by Michael Harris, we see how an increasingly constant interaction with, reliance on, and addiction to technology is creating devastating effects on us neurologically.
In my book review of The End of Absence by Michael Harris, we see how an increasingly constant interaction with, reliance on, and addiction to technology is creating devastating effects on us neurologically.
Among these effects are dementia-like symptoms: loss of short-term memory, easy distraction, lack of focus, loss of critical thinking skills, and loss of executive functions.
These effects are happening to people all around us just like you and me. The effects don’t discriminate: even the very young are affected just as profoundly as others of varying ages.
In Nicholas Carr’s The Shallows: What the Internet is Doing to Our Brains, a book everybody should read, the discussion centers on the neurological effects of 24/7 technology connection in the actual composition of the brain.
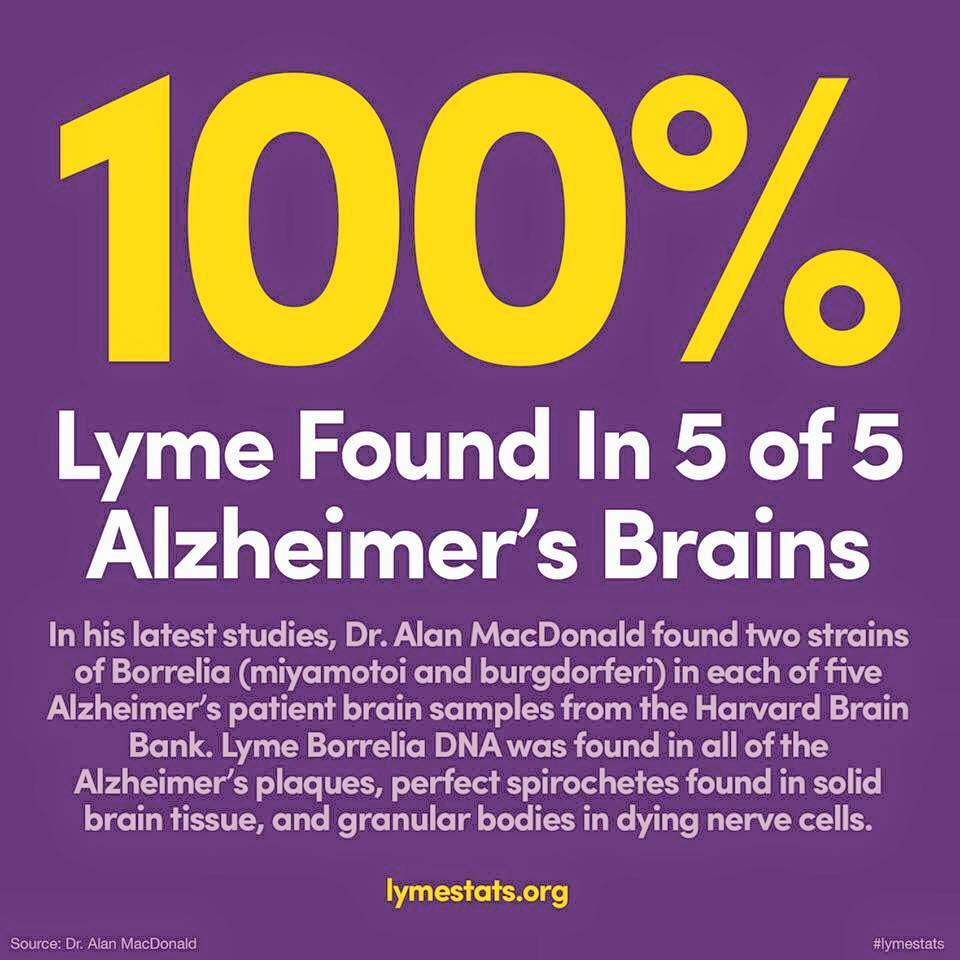
The research and the science is sobering, especially in light of how it points to the emergence of another lifestyle dementia that is already beginning to affect people, and will increasingly affect vast numbers of people at earlier and earlier ages.
Lifestyle dementias are dementias we choose because we adopt or don’t control or eliminate the lifestyle factors that cause the dementias.
Alcohol abuse and addiction is one of those lifestyle choices. How we treat our bodies (food, exercise, etc.) is another lifestyle choice. The quality and quantity of our sleep is yet another lifestyle choice.
And our relationship with technology presents even one more lifestyle choice. A recent Pew Research Center survey revealed that 20% of Americans report that they are online almost constantly.
That is 1 in every 5 people here in the United States. It is not surprising to me, but it is disturbing to me for many reasons.
Because my whole career has been intricately involved with technology, I’m uniquely qualified to discuss this since I’ve always made choices to limit my exposure, instinctively, I suppose, realizing the dangers, and I continue to do so because my brain, for better or worse, is the best asset I have and I don’t want my choices to be the reason I lose any functionality it has.
 Overexposure to technology completely rewires our brains (neuroplasticity) and not in positive ways. It literally changes our neural pathways, eliminating the ones we don’t use and creating new ones.
Overexposure to technology completely rewires our brains (neuroplasticity) and not in positive ways. It literally changes our neural pathways, eliminating the ones we don’t use and creating new ones.
Different parts of the brain are stimulated with how we receive information.
Images light up a different area of the brain than words do. Technology lights up a totally different area of the brain than either images or words do.
Which area of our brains get lit up the most often is the part of the brain that becomes dominant and we use the other parts less and less.
 With disuse, those parts we don’t use begin to die at the cellular level, eventually creating the same kinds of synaptic gaps that are common among dementias.
With disuse, those parts we don’t use begin to die at the cellular level, eventually creating the same kinds of synaptic gaps that are common among dementias.
The brain is the only organ in which there is no cellular regenation. Once the cells in the brain die, they’re gone for good. With time, this cellular death becomes widespread and we experience dementia.
The problem with our increasing interaction exclusively with technology (smart phones and tablets have definitely made this easier) is that technology is purposefully designed to stimulate the part of the brain that deals with emotions.
Because of the emotional stimulation that technology elicits, it consistently bypasses logical, analytic processing of information and the desire and ability to discern between what’s true and false, what’s right and wrong, and what’s valuable and what’s not.
The effect on us is that we are unaware of what’s happening  behind the scenes to our brains as we’re tethered to technology, so we don’t realize we’re not logically and analytically processing information coming in and that we’re rapidly losing the desire and ability to discern between what is true and false, what is right and wrong, and what is valuable and what is not.
behind the scenes to our brains as we’re tethered to technology, so we don’t realize we’re not logically and analytically processing information coming in and that we’re rapidly losing the desire and ability to discern between what is true and false, what is right and wrong, and what is valuable and what is not.
It is simply disappearing without our awareness that we’re losing the very things that make us unique as humans and which are the most precious gifts we have been given.
The end result is that in the short term we become shallow (gullible, unthinking, ignorant, and imprisoned in a shrinking world that is simply a mirrored reflection of our narcissistic selves) and in the long term that we lose our cognitive abilities altogether.
It’s not to late for most of us to turn this around and do everything in our power to make choices that will stave off this lifestyle dementia.
But each of us has to make the choice for ourselves. Some of us won’t. Some of us don’t believe this is happening. Some of us don’t care.
However, for those that will, that do believe this is happening, and that do care, here are a few ways to get started:
- Unplug from everything at a set time every day and stick to it. Replace the time that you would have spent with technology with an activity that involves the other parts of your brain. These can include hobbies, reading, putting together jigsaw puzzles, playing board games or cards with other people, crossword puzzles, sudoku, and other types of brain-intensive puzzles.
- Don’t stay plugged in all day. Do what you need to do (check social media, email, texts, etc.) at set time-delimited times each day (I generally check mine early morning, noon, and 6 pm, giving myself 15 minutes each time and no more). Otherwise, I’m off the grid and working on other productive things.
- Unplug completely for 24 hours each week. No phone, no internet, no social media, no nothing. And do something else entirely away from it all. This may, especially if we’re addicted to technology, be quite uncomfortable and unsettling at first (generations before us lived this way and they not only survived just fine, but I suspect they were happier and better off), but eventually you will absolutely crave your unplugged 24 hours and it may lead you to more complete unplugging than that in time.
We only get one brain in our lives. Everything we do supports it or destroys it. Once destruction happens, it’s permanent and it can’t be undone.
Let’s make sure we’re doing everything in our power with our choices to support our brains and not destroy them.