We humans are a very gullible bunch. We are also capable of the most incredible leaps of faith in tying the most disparate and thinly-threaded information together while we routinely disbelieve proven facts and credible information backed by proof, analysis, and critical thinking.
We humans are a very gullible bunch. We are also capable of the most incredible leaps of faith in tying the most disparate and thinly-threaded information together while we routinely disbelieve proven facts and credible information backed by proof, analysis, and critical thinking.
Why is that we go to the outermost reaches of implausible information to build our internal knowledgebases on instead of doing real, credible – yes, it takes time, it takes effort, it takes analysis, it takes critical thinking, it takes patience, and it takes commitment – research to understand the various kinds of dementa (Alzheimer’s is just one kind of dementia), to understand what the scientific process – and effects are – and to understand how we as caregivers can love and support our loved ones with honor and dignity?
Going Gentle Into That Good Night is a comprehensive resource for factual, well-researched, and practical information on dementias. The information is free for everybody. Yet routinely I see the most outlandish and untrue information on dementias on social media.
Silver bullet cures (there are no cures). Unproven links to other diseases based on an infinitesimally small test sample (no real scientist or pathologist would hang their careers on samplings this small to announce a finding). Claims that this or that “natural” thing will reverse or improve a brain already neurologically compromised.
It sounds wonderful. But it is misinformation, disinformation, and, in many cases, completely dishonest.
For a lot of these things, the motive is to get us to spend a lot of our hard-earned money on a pipe dream while the people getting rich on our backs are laughing all the way to the bank. For the other things, it is simply a matter of hacks or inferior scientists, doctors, etc. trying to get their 15 minutes of fame.
All at our expense and at the expense of our loved ones with dementias and Alzheimer’s Disease. Not only is there a monetary expense, but there is also an emotional expense, a psychological expense, and a physical expense.
All of these areas can be significantly drained and irreparably damaged in the process.
 An example of this insanity in the pre-information age was in the widespread usage of mercury as a cure-all during the 18th and 19th centuries. Mercury, it turns out, is incredibly toxic and rapidly leads to premature death (Louisa May Alcott, author of Little Women, died an early death from mercury, which was prescribed for her various physical ailments, poisoning).
An example of this insanity in the pre-information age was in the widespread usage of mercury as a cure-all during the 18th and 19th centuries. Mercury, it turns out, is incredibly toxic and rapidly leads to premature death (Louisa May Alcott, author of Little Women, died an early death from mercury, which was prescribed for her various physical ailments, poisoning).
It is easy to think, “Duh!” now, but the same kind of misinformation, disinformation, and outright lies are even more rampant and accessible today because of technology.
If you want to believe something – even something unproven, outrageous, dead wrong, and possibly life-threatening – the internet offers you the backup and the “proof” you need to justify whatever it is you want to believe.
The internet is full of hacks. It is full of wannabes. It is full of misinformation, disinformation, and lies. About dementias. And about everything else.
Do not believe anything that you cannot prove yourself beyond a shadow of a doubt. Do not trust anything just because it looks like somebody credible (a doctor, perhaps) said it.
I implore you not to check your critical thinking, your BS meter (we all have one, I hope), your logic, your reason, and your common sense at the door when you enter the wild and wacky world of the internet.
Here’s the most important thing to remember. Most disinformation, misinformation, and outright lies have a tiny grain of truth in them. That is always the hook. Always.
However one grain of truth surrounded by countless grains of not truth still makes the information as a whole untrue. Do not fall for the hook because once you do, then you are moving as far and as fast away from the truth as possible.
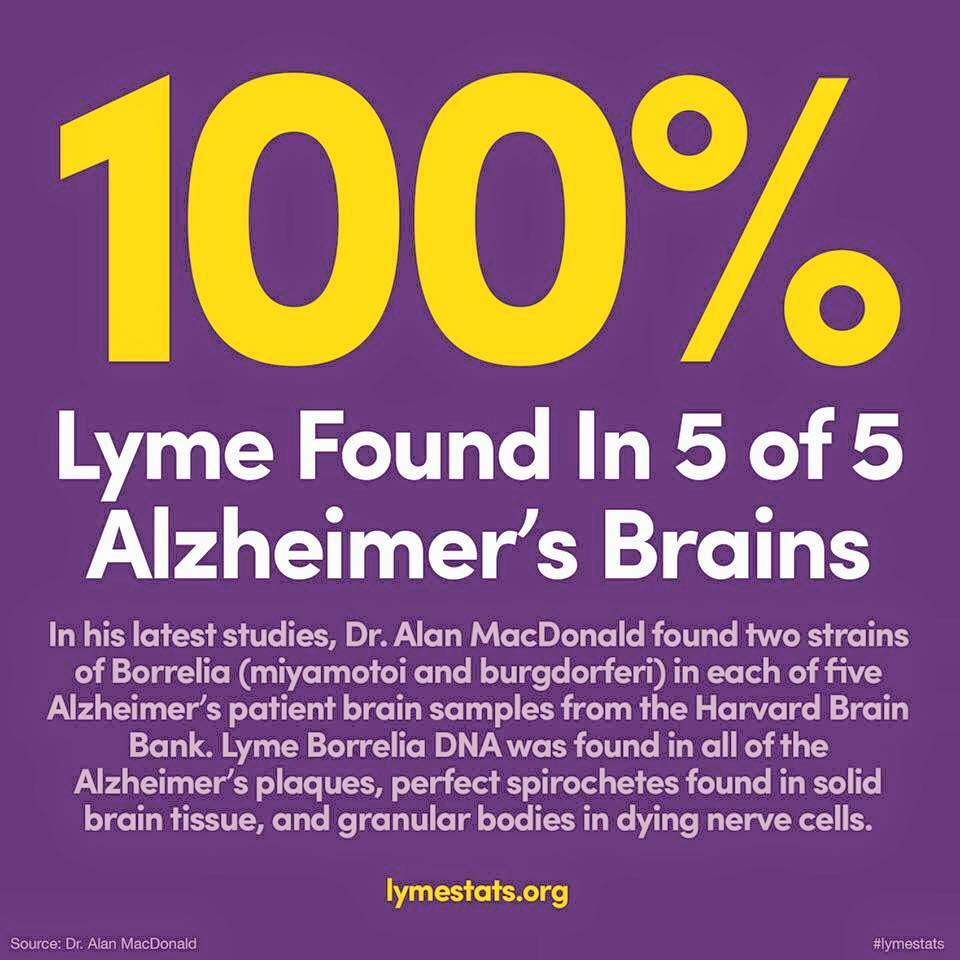
 An example related directly to dementias is the supposition that shows up over and over that Lyme Disease is the cause of Alzheimer’s Disease.
An example related directly to dementias is the supposition that shows up over and over that Lyme Disease is the cause of Alzheimer’s Disease.
This is sensational disinformation and misinformation. A healthy dose of common sense with thoughtful, careful, and diligent research, analysis, and critical thinking would prove or disprove this bombshell claim.
Common sense brings the “5 in 5 brains” into focus. Five brains out of the millions of people who have had and who have some form of dementia is not a credible sampling of the population affected.
I could very easily go out and find five random people who have the same auburn hair that I do and declare that I have turned genetics upside down and found that auburn hair is a dominant trait (it is recessive).
This is common sense and logic and we must bring these to the table when we’re looking at any and all information. Applied to this graphic, we should automatically mistrust this information.
But that’s not enough to prove it wrong. We actually have to go and do some research. This microstudy was done by McDonald in 2006. The opening statement of the abstract tells us key information through which to view McDonald’s microstudy: “Here is hypothesized a truly revolutionary notion…”
A hypothesis is not fact. It is a theory, a guess, an imagination that remains to be proved or disproved. The infographic, then, presents the information as already being proved, which is misinformation.
That the study was done almost 10 years ago also raises the eyebrows of doubt because much has been done in the research and causes of dementias and Alzheimer’s Disease in those intervening years.
In fact, with some research on the possible link between Lyme Disease and Alzheimer’s Disease, we find a study from 2014 (eight years after McDonald’s microstudy) that definitively repudiates the existence of a link between the two diseases.
To not verify and prove anything and everything is not only lazy, but in many ways, ignorant. Why would we not want to get all the facts instead of trying to support some pet theory that we believe? I don’t understand that.
Too few of us, to our discredit, actually go through this process and that is what I am begging each of you and imploring each of you to do. Know why you know what you know. Know why you believe what you believe. Know why you do what you do.
Never, ever accept anybody else’s word for anything. Prove it. Disprove it. But never just accept it.
Ever. If not for ourselves, for our loved ones. They’ve entrusted their lives to us. We owe it to them to be rigorously honest and apply that everywhere in our lives and to not fall for gimmicks, misinformation, disinformation, and outright lies.
The cost of not doing this is high to everyone.
To us in terms of our character and our credibility (if we perpetuate disinformation, misinformation, and erroneous information, then we are leading people astray and away from the truth).
To our loved ones in terms of their care and their lives (we can cause much harm and much suffering by believing things that are not true and not proven).
A huge part of true love is the continuous hard work it requires us to put into living it, being it, showing it consistently and continually.
Is our love real or is it not? How do we know?
 Today, February 7, 2016, the 50th Super Bowl game in NFL (National Football League) history will be played by the Carolina Panthers and the Denver Broncos. Therefore, it is appropriate to discuss the other dark and dangerous side of this football game – and all the ones played before and all the ones that will be played after – before it is played.
Today, February 7, 2016, the 50th Super Bowl game in NFL (National Football League) history will be played by the Carolina Panthers and the Denver Broncos. Therefore, it is appropriate to discuss the other dark and dangerous side of this football game – and all the ones played before and all the ones that will be played after – before it is played.